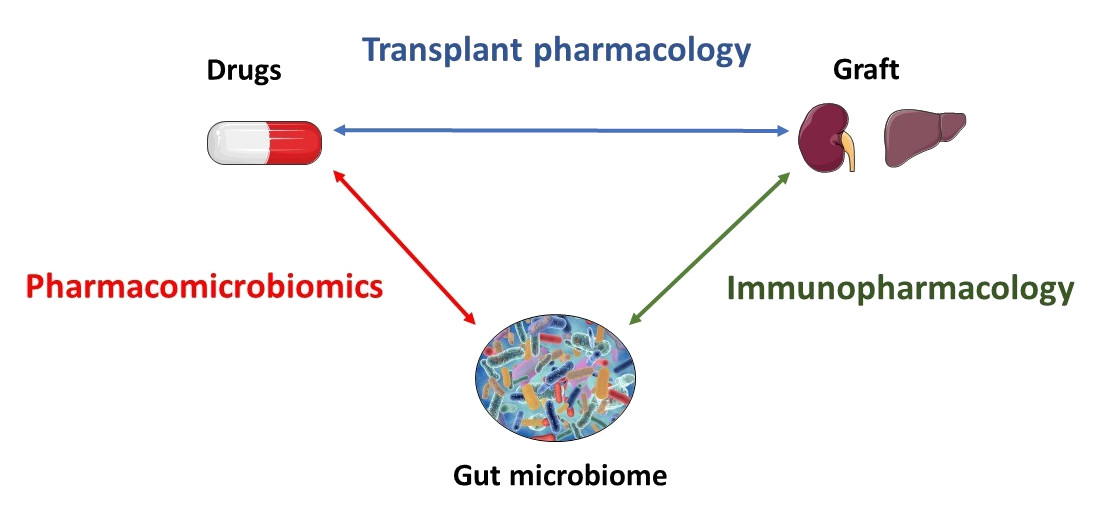
Our unit is dedicated to precision medicine in transplantation by merging multi-scale knowledge and research on immunosuppressive drugs. In this perspective, our team investigates gut microbiota-host-immunosuppressant drug interplay and its contribution to the interindividual variability of transplant outcomes. Therefore, we are therefore conducting several projects in the field of pharmacomicrobiomics and immunopharmacology.

Roland Lawson
Project manager
|
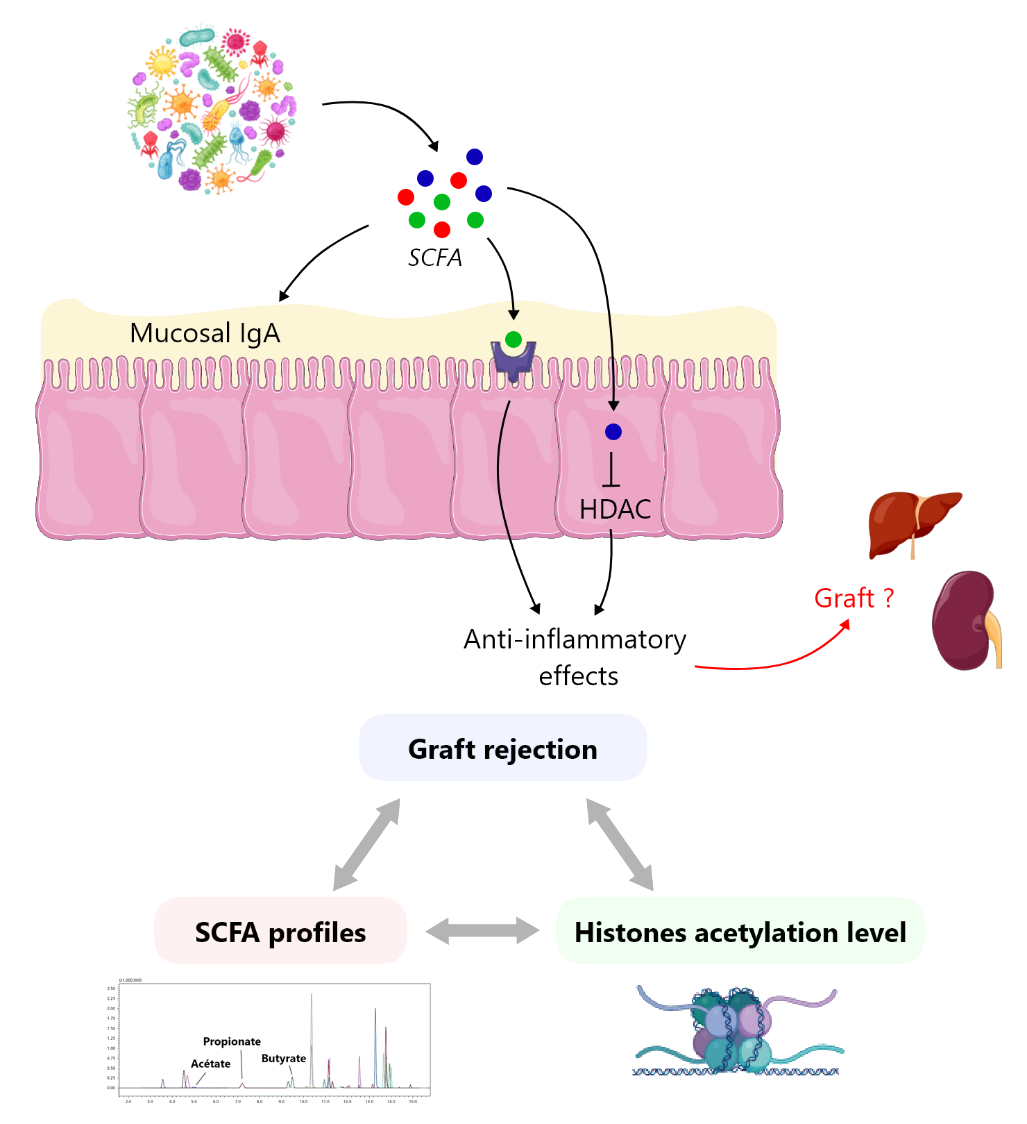
Immunosuppressive drugs are known to induce modifications in the gut microbial community. Gut microbiome plays a central role in shaping the host immune system, particularly the production of the main mucosal immunoglobulin IgA. Gut microbiome modulation (so-called dysbiosis) has been linked to transplant outcomes. Dysbiosis can affect the ability of specific bacterial populations to produce short-chain fatty acids (SCFA), which are crucial for host homeostasis. Epigenetics have shed light on the possible involvement of SCFA (e.g., acetate, propionate and butyrate) in post-translational histone modifications such as acetylation. It is worth mentioning that histone modifications have been associated with malignant or autoimmune diseases suggesting a very plausible role in immunity modulation of the transplanted patient. Histone acetylation is generally associated with increased transcriptional activities owing to a higher accessibility of DNA double strand to transcription factors. SCFA prevent histone deacetylation by inhibiting histone deacetylases (HDAC). This is particularly true for butyrate, which is the most potent HDAC inhibitor (HDACi) amongst SCFA. Interestingly, HDACi have demonstrated their therapeutic potential in oncology, as well as for the treatment of autoimmune diseases. However, to date, only very few studies have investigated the correlation between dysbiosis, SCFA profile and graft rejection. The present project aims (i) to explore the causal link between graft rejection and SCFA level and (ii) to assess the therapeutic potential of either food supplementation with SCFA or HDACi in order to prevent graft rejection. We will evaluate the link between the longitudinal evolution of SCFA concentrations in plasma and urine samples from a retrospective cohort of transplant patients and episodes of graft rejection. |
 |
| Organ transplantation strongly depends on the initial quality of the graft, which in turn depends on various parameters, e.g., donors characteristics and conditioning, organ harvesting procedures, and organ preservation protocols. In order to face the growing need for organs from a limited number of living or brain-dead donors, most of the organ removal centres have increasingly used sub-optimal donors. In this context, the organs retrieved are more prone to ischemia-reperfusion (IR) injuries. IR is a complex pathophysiological process associated with numerous structural and metabolic modifications potentially leading to either short or long-term graft failure, in the form of acute rejection, chronic allograft nephropathy and ultimately graft loss of function. Using a preservative approach during the conservation period might help to prevent or at least to minimise the consequences of IR injuries. Short chain fatty acids (SCFA), and more specifically butyrate, represent a source of energy in many cell types. They have also demonstrated protective effects against IR injuries. This project aims to evaluate the protective effect of SCFA supplementation in organ preservation fluids using cellular and mouse models. | 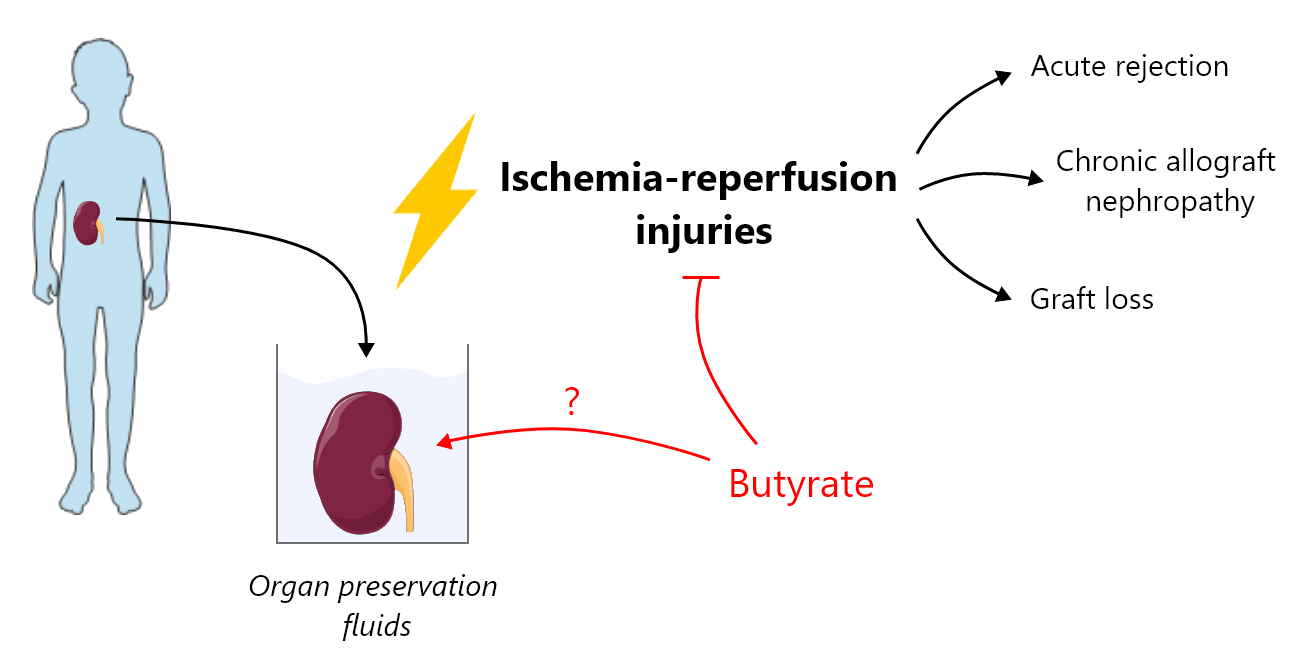 |
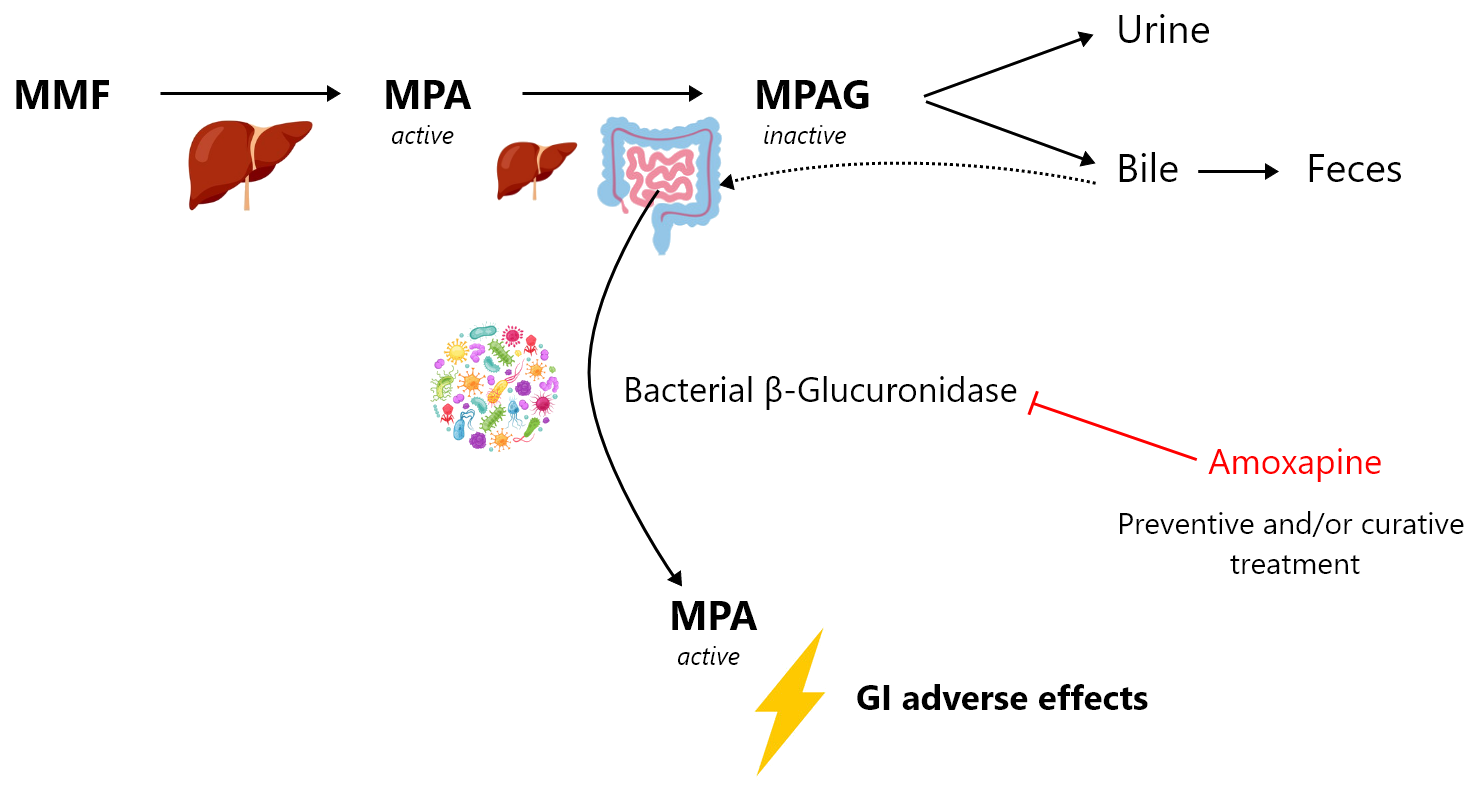
Mycophenolate mofetil (MMF) is one of the most effective immunosuppressants. It is widely used in solid organ and bone marrow transplantation as well as in autoimmune disorders (e.g., lupus erythematosus, rheumatoid arthritis, psoriatic arthritis or vasculitis). MMF treatment is unfortunately associated with multiple adverse effects, among which the gastrointestinal effects are of major concern. More than 30% of patients complain of gastrointestinal adverse effects, which can range from simple nausea, vomiting, abdominal pain or diarrhoea to bleeding ulcerations and erosions of the gastrointestinal tract. They can occur regardless of MMF exposure duration, leading to a significant decrease of patient adherence to the treatment. These gastrointestinal adverse effects of MMF are likely to be mediated by the intestinal back-transformation of the metabolite mycophenolic acid glucuronide (MPAG) excreted by the hepatocytes in bile, into the active parent form mycophenolic acid (MPA). Bacterial β-glucuronidase (β-G) expressed by certain bacterial phyla found in the microbiome are able to transform MPAG into MPA. Thus, a change in the intestinal microbiota or intestinal dysbiosis in transplanted patients, which may favour the proliferation of bacteria expressing this enzyme or induce its expression, are likely to result in increased concentrations of MPA in the distal intestine, resulting in turn in gastrointestinal adverse effects.
Our project aims to evaluate the effect of the targeted inhibition of bacterial β-G as a preventive and/or curative treatment of MPA-induced gastrointestinal damage. We will evaluate, in a mouse MMF-induced colitis model, the therapeutic potential of a selective bacterial β-G inhibitor, amoxapine. Amoxapine is an antidepressant used in human that is also a potent inhibitor of bacterial β-G with no antibiotic effect. In parallel, we will characterize new candidate inhibitors of bacterial β-G by means of high-throughput screening of a large academic chemical library. This approach will be supported by atomic-scale thermodynamic modelling of β-G inhibition.
|
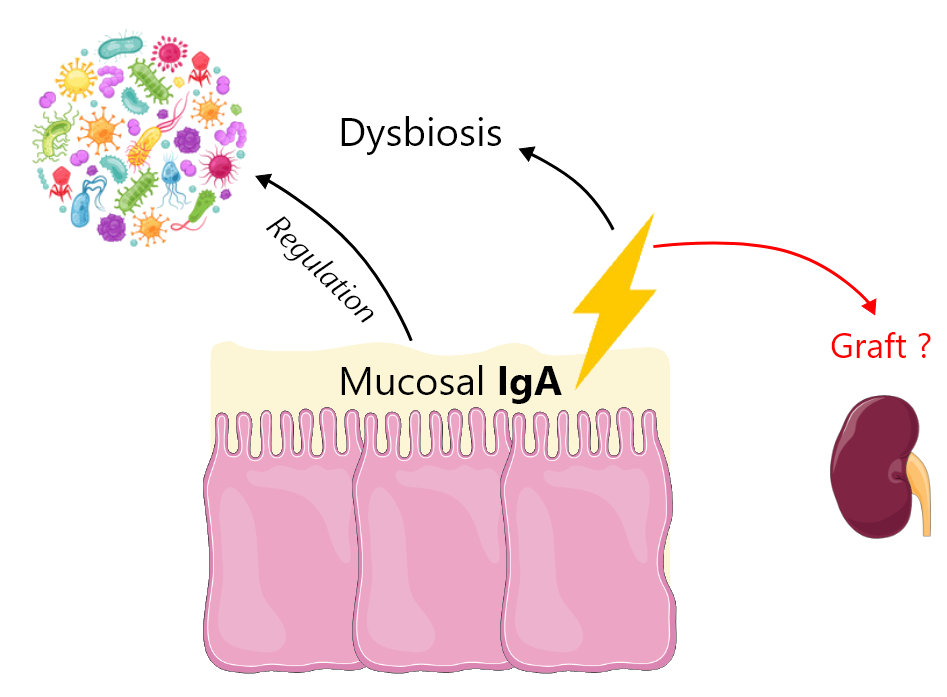
Immunoglobulin A (IgA) is the predominant isotype in mucosa secretions, where it plays a major role in the regulation of the microbiota. Deficient IgA production by the mucosa or transport into the intestinal lumen leads to dysbiosis in mice. Selective IgA deficiency, usually asymptomatic and fortuitously discovered based on IgA blood level, is the most frequent primary immunodeficiency in humans, with an estimated prevalence of 1:700 individuals of European descent. Recently, it has been shown that IgA-deficient humans present gut microbiota dysbiosis. The most frequent IgA disease, the IgA nephropathy is also characterized by microbiota dysbiosis. IgA nephropathy is the most common primary glomerulonephritis in the world with a prevalence of 10% in European countries. Usually IgA nephropathy is benign; however, in 25% of patients, it leads to end-stage renal failure requiring renal function replacement. It is characterized by abnormal circulating IgA, potentially due to an anomaly of mucosal IgA production, and IgA deposition in the glomeruli. Studies in transplanted patients with primary IgA nephropathy showed that kidney graft survival is not statistically different in these patients as compared to those with other primary kidney diseases, despite microbiota dysbiosis. The aim of this project consists in evaluating the impact of individual IgA status, i.e. IgA-normal, IgA-deficient or IgA-abnormal (IgA nephropathy), on graft outcome and MMF adverse effects. Two approaches will be used: mouse models and analysis of retrospective samples and clinical data from a cohort of transplant patients. |
 |